


Dear Readers,
This article will discuss the functions and dysfunctions of Testis (Part-1) and in a subsequent article we will highlight the scientific evidence of how mindful yoga and meditation can help us to balance the dysfunctional testis (Part-2).

The TL;DR
Testes in males are analogous to the female ovaries.
Main functions involve production of sex hormones like, testosterone, anti-mullerian hormone, inhibin B, estradiol and production of sperms.
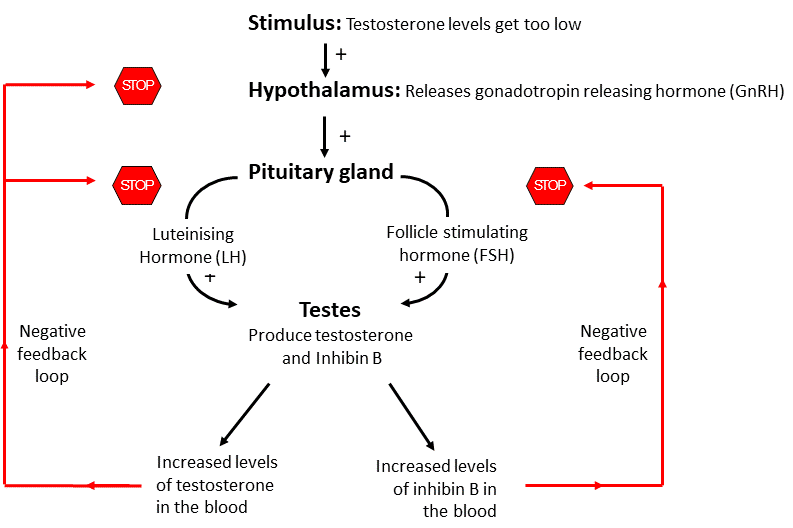
Hormone levels in blood are under tight regulation of hypothalamus-pituitary-testes (HPT) axis.
Testes abnormalities include: Hypogonadism, Cryptorchidism, Testicular Cancer, Male Infertility
The best way to maintain testosterone levels during the transition from middle to older age is to engage in healthy lifestyle behaviours
Let’s dive deeper….
(According to Kundalini Yogis: Svadhisthana or sacral chakra)
1.1 Testis
Testis in males are analogous to the female ovaries. They produce sex hormones called androgens (primarily testosterone) and are the place for the production of sperm (spermatogenesis).
Anatomy: Testis are ovoid in shape, sized four to six centimeters in length. They descend to scrotum before birth and are attached to it by the testicular ligament while remaining connected with the abdomen by spermatic cords.
The testis is made up of 200-300 compartments called lobules. Each lobule contains several coiled structures called seminiferous tubules, where sperm are made. These tubules are lined with epithelium layer which is made up of Sertoli cells that aid in the production of hormones and testicular fluid, which are essential for the development of the spermatozoa or sperm cells. Among these Sertoli cells there are spermatogenic cells that divide and form sperm cells.
Around the seminiferous tubules are the specialised male androgens secreting Leydig (interstitial) cells, especially testosterone. Their cytoplasm is rich in cholesterol-lipid droplets. Cholesterol is used in the first step of testosterone production. The Leydig cells make and secrete testosterone, in response to lutenising hormone (LH) from the pituitary.
Did You Know? Cholesterol is needed for Testosterone production, but that doesn't mean that having high cholesterol will result in high testosterone levels.
There are also squamous contractile cells called myoid cells surrounding the basement membrane, which generate peristaltic waves in the tubules.

1.2 Endocrine Functions of Testes
Endocrine function, i.e. production of hormones does not start until puberty when LH stimulates the Leydig cells to produce testosterone.

Testosterone
Testosterone is the main male hormone which is also present in women but in much smaller amounts as compared to men. Testosterone can be converted into a more active male sex hormone, called dihydrotestosterone.
It plays a number of important roles, such as:
The development of the penis and testes
The deepening of the voice during puberty
The appearance of facial and pubic hair starting at puberty
Play a role in balding
Muscle size and strength
Bone growth and strength
Sex drive (libido)
Sperm production
Did You Know? Testosterone's role in bad behaviour is largely a myth.
Problems associated with abnormally high testosterone levels are seen in athletes who either use anabolic steroids, testosterone or related hormones to increase muscle mass and their performance.
Symptoms of high testosterone levels include:
Low sperm counts, shrinking of the testicles and impotence
Heart muscle damage and increased risk of heart attack
Prostate enlargement with difficulty urinating
Liver disease
Acne
Fluid retention with swelling of the legs and feet
Weight gain, perhaps related in part to increased appetite
High blood pressure and cholesterol
Insomnia
Headaches
Increased muscle mass
Increased risk of blood clots
Stunted growth in adolescents
Uncharacteristically aggressive behavior (although not well studied or clearly proven)
Mood swings, euphoria, irritability, impaired judgment, delusions
During the course of a day and over time levels of testosterone vary dramatically. As men age, testosterone levels drop very gradually, about 1% to 2% each year. This is in contrast to women’s sex hormone (estrogen) levels which drop sharply at menopause. More than a third of men over 45 years may have reduced levels of testosterone than might be considered normal.
The best way to maintain testosterone levels during the transition from middle to older age is to engage in healthy lifestyle behaviours and avoid excess weight gain.
Symptoms of testosterone deficiency in adult men include:
Reduced body and facial hair
Loss of muscle mass
Low libido, impotence, small testicles, reduced sperm count and infertility
Increased breast size
Hot flashes
Irritability, poor concentration and depression
Loss of body hair
Brittle bones and an increased risk of fracture
Anti-Mullerian hormone (AMH)
This hormone plays important role for sex differentiation in the unborn baby during early pregnancy. It shuts down the development of female ducts which later develops into fallopian tubes, uterus and vagina. AMH thus allows for the development of male reproductive organs like epididymis, vas deferens and the seminal vesicles of the testes.
Estradiol
Leydig cells also produces estradiol though in much smaller amounts as compared to women. In men, estradiol contributes to bone health and helps in the maturation of sperm.
Inhibin B
This hormone is released from the Sertoli cells and it plays crucial role in the HPT axis. Increased levels of Inhibit B in the blood initiates the negative feedback loop, signals the pituitary to decrease the FSH levels.
1.3 Hypothalamic-pituitary-testicular (HPT) axis
Hormone levels in blood are under tight regulation of HPT axis. When testosterone levels rise low, hypothalamus releases gonadotropin releasing hormone which then signals to the pituitary gland at the base of the brain to release Lutenising hormone and Follicle Stimulating Hormone which then relays signals to the testes to produce testosterone. A "feedback loop" closely regulates the amount of hormone in the blood. When testosterone levels rise too high, the testes sends signals via release of Inhibin B to the pituitary to reduce production.
1.4 Endocrine Testes Abnormalities
1. Hypogonadism
A condition where the testes are unable to produce enough testosterone (called androgen deficiency) and/or a normal number of sperm.
Primary hypogonadism: Primary hypogonadism results from conditions affecting the testes, resulting in androgen deficiency and reduced fertility. This includes:
Undescended testes
Absent testes (anorchidism)
Infections (e.g. mumps)
Testicular injuries
Tumors
Cancer treatment (chemotherapy or radiotherapy to the testes)
Genetic conditions such as Klinefelter’s syndrome (a genetic condition that results when a boy is born with an extra copy of the X chromosome).
Secondary hypogonadism: caused by conditions that affect the hypothalamus and/or the pituitary gland. In these cases, the testes do not receive the signals to make testosterone and sperm.
Other causes may include older age, obesity, other health conditions and medications or abuse of anabolic-androgenic steroids
What is the relationship between obesity and lower testosterone levels?
Moderate obesity predominantly decreases total testosterone due to insulin resistance-associated reductions in sex hormone binding globulin. More severe obesity is additionally associated with reductions in free testosterone levels due to suppression of the hypothalamic-pituitary-testicular axis. Besides obesity is associated with increased mortality primarily due to increased risk of cardiovascular disease and type 2 diabetes mellitus and increased morbidity from arthritis and sleep-related breathing disorders. During COVID19 pandemic, epidemiologists have seen that obese individuals are also at higher risk of getting severe COVID disease.

Low testosterone levels are associated with increased fat mass (particularly central adiposity) and reduced lean mass in males. Thus, this bidirectional relationship between testosterone and obesity creates a self-perpetuating cycle of metabolic complications. However, reducing body weight, BMI, and most importantly central adiposity (waist circumference), levels of testosterone can be increased and thus complications related to low testosterone levels can be reversed like erectile dysfunctions etc.

2. Cryptorchidism
Condition when testicles are undescended, i.e. hasn't moved into scrotum before birth. It is uncommon condition, usually happens in baby boys born prematurely. Most of the times only one testicle is affected, but about 10 percent of the time both testicles are undescended. Exact cause of cryptorchidism is not clear, it is thought that genetics, maternal health and other environmental factors might play a role in disrupting the hormones, physical changes and nerve activity that influence the development of the testicles.
Undescended testicles are also linked to a higher risk of:
Testicular cancer in adulthood (though the risk is still less than 1 in 100)
Testicular torsion (twisting of the chord that brings blood to the scrotum)
Developing a hernia near the groin
3. Testicular Cancer
Testicular cancer starts in testis. Though it can affect a man or boy at any age, it is most often found in men age 15 to 44 years. It’s fairly rare and very treatable. With early diagnosis, testicular cancer can be cured.
Signs of a testicular tumor are:
A painless lump in the testicle (the most common sign)
Swelling of the testicle (with or without pain) or a feeling of weight in the scrotum
Pain or a dull ache in the testicle, scrotum or groin
Tenderness or changes in the male breast tissue
It is vital to reach out to a urologist if you notice any of above signs. This is especially true if a sign lasts for more than two weeks.
4. Male Infertility
Male infertility is any health issue in a man that lowers the chances of his female partner getting pregnant.
There can be many underlying reasons for male infertility, some of the causes are:
Sperm Disorders (oligospermia: sperms made in very low numbers or azoospermia: not made at all, oddly shaped, slow movement etc)
Varicoceles (swollen veins in the scrotum which blocks proper blood drainage and thus results in perturbing sperm growth)
Retrograde Ejaculation (semen goes backwards in the body)
Immunonologic Infertility (when man's body makes antibodies that attack his own sperm)
Obstruction (the tubes through which sperm travel can be blocked)
Hormones
Medication
Certain medications can change sperm production, function and delivery. These medications are most often given to treat health problems like:
arthritis
depression
digestive problems
anxiety or depression
infections
high blood pressure
cancer
Male infertility is heterogeneous, complex, and often multifactorial. A strong evidence is emerging to support the idea that men with infertility and their family members are at an increased risk of developing various malignancies.
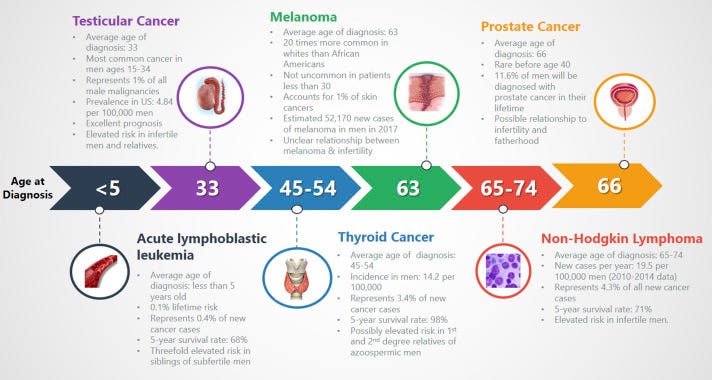
Source: Article
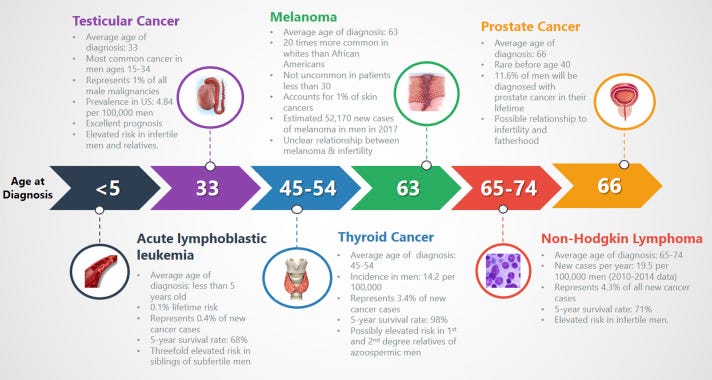
However, a more thorough understanding of the impact of genetics and epigenetics (the study of how your behaviours and environment can cause changes that affect the way your genes work) on infertility will likely elucidate mechanistic pathways that connect infertility to cancer.